- Visibility 18 Views
- Downloads 4 Downloads
- DOI 10.18231/j.jco.2025.012
-
CrossMark

Comparative evaluation of accuracy for manual, digital and cbct generated superimposition of cephalometric landmarks- A retrospective study
- Author Details:
-
Ibrahim Chinde
-
Ajit Kalia
-
Salil Nene
-
Tanuja Rankhamb
-
 Sakina Abbas Rampuri *
Sakina Abbas Rampuri *
Introduction
The essence of clinical orthodontics is the supervision, guidance, and correction of the growing dentofacial structures.[1], [2], [3] Since the 1970s, lateral cephalometrics has been the gold standard for evaluating the facial skeleton's relationship to the dentition for orthodontic and orthopedic treatment planning.
A superimposition[4] is an analysis of the same patient taken at different times. It is used to assess changes in the dentoalveolar and basal connections during a course of orthodontic or surgical treatment, as well as changes in a patient's growth pattern over time. Various methods of superimposition have been developed over time, including the Decoster method, which uses the bony anatomy of the front contour of the cranial base to support the superimposition Broadbent triangle. The Sella-nasion[5] line provides a complex view of growth change, while the Basion-Nasion plane by Coben is used as a reference point for overall dentofacial change evaluation. The superimposition area of the Ba-Na line with registration at the CC point helps to evaluate changes in the facial axis, the direction of chin growth, and the upper molar position. [4] The American Board of Orthodontics (ABO) has adopted the maxillary anatomical method by recommending registering ‘‘on the lingual curvature of the palate and the best fit on the maxillary bony structures to assess maxillary tooth movement.
Despite the extensive use of cephalometric radiographs, they have various limitations, such as projection errors, magnification variations, imaging artifacts, information voids, and errors in head posturing.[1], [2], [6] As a result, the area of dental orthodontics has moved more and more toward digitization. CBCT data sets offer undistorted 3D morphology, enabling the identification of craniofacial structures more naturally, especially in cases involving impacted teeth, facial asymmetries, or craniofacial anomalies.[7] Unlike conventional cephalograms, CBCT allows for the correction of errors due to incorrect patient positioning during image acquisition through interactive adjustments. With the accuracy and reliability associated with 3D superimpositions, clinicians have a useful method for evaluating orthodontic treatment changes as well as growth in patients who require CBCT imaging.[8]
Computer-assisted cephalometric analysis uses digital tracing to calculate angles and distances, eliminating errors in drawing lines between landmarks.[9] The computerized digital analysis program is user-friendly, efficient, and saves time by allowing quick measurements, simultaneous analyses, image retention, and less storage space. It also aids in superimposition, image size and contrast adjustment, and image archiving. It also allows for image superimposition, image size, contrast adjustment, and improved access to images.[10] However, it requires a costly digital cephalometric radiographic machine and software.[3] The gold standard for cephalometric evaluation is yet to be defined, and traditional imaging methods are questioned due to errors, time consumption, and limitations in bi-dimensional diagnosis.
In this retrospective study, the accuracy of manual, digital, and CBCT-generated superimpositions of various cephalometric landmarks were evaluated and compared using Dolphin and INVIVO softwares.
Materials and Methods
The present study consisted of 20 selected lateral cephalograms and CBCT scans from the pre-existing database at the Department of Orthodontics and Dentofacial Orthopedics. The ethical committee reviewed and approved all the sample sizes and selection criteria for the study.
The Lateral cephalograms were obtained from the same cephalostats, utilizing identical software and a workstation, and maintained under consistent environmental conditions. The distance between the patient's head's mid-sagittal plane and the X-ray source was consistently kept at 5 feet, using an 8 X 10 inches film. The subjects were positioned in the cephalostat with the sagittal plane perpendicular to the X-ray path, and the Frankfort plane parallel to the floor, establishing occlusion in centric occlusion. The exposure parameters were fixed at 82KVp, 12mA, for a period of 0.8mins seconds.
The 20 CBCT scans were acquired from a Carestream CS9300 machine, with all patients scanned using the same Carestream 3D imaging system, featuring specific scan settings: 87kV, 8 mA, 17cm * 13 cm field of view, 0.5 mm voxel size, and a scanning time of 11.3 seconds per section.
Inclusion Criteria for selection of Lateral cephalogram and CBCT scans
Full complement of teeth up to second molar should be essentially present
Absence of any periapical pathologies
The radiographs should be devoid of any artifacts, Patient without metal prostheses to avoid streak artifacts.
The dentition should be in centric occlusion and the lips should be in a relaxed position
No craniofacial deformity or asymmetry
There should not be any excess soft tissue that could potentially interfere with the location of anatomical points.
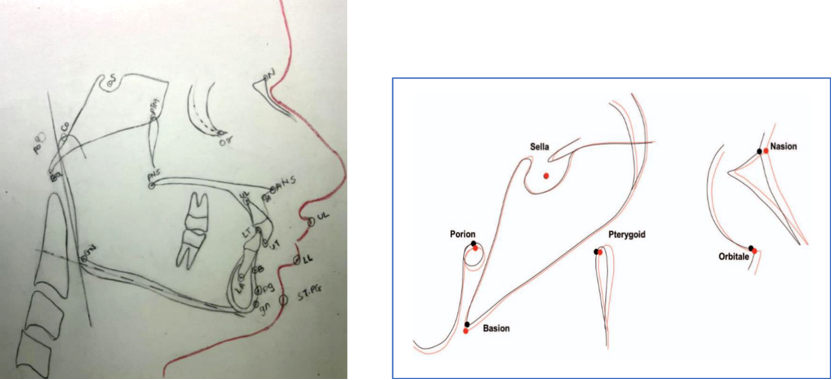
Method of conventional hand tracing: Conventional hand tracing was performed in a darkened room using a tracing table screen on a fine transparent acetate paper of 0.003 inches. Landmarks were identified by a single point, in a predetermined order, and for bilateral structures and double images, the mid-point was chosen by construction. The values obtained from manual tracing were considered as the control group for the study.
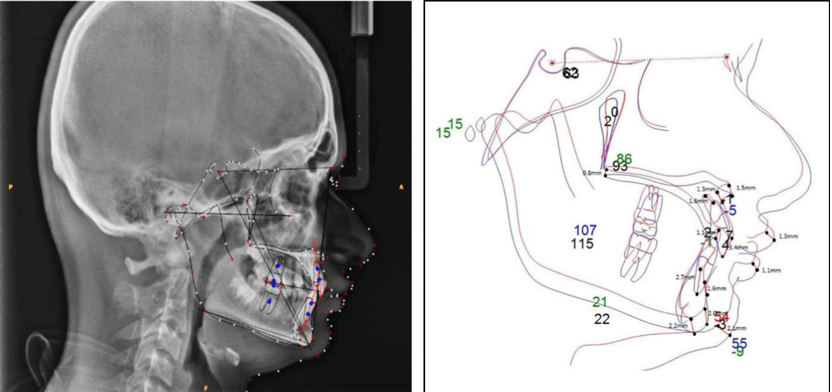
Method of Computerized Digital tracing: All the digital images JPEG were directly imported into software programs and calibrated by digitizing two points on the ruler which was inbuilt in the cephalostat. During the identification of landmarks, the digital image enhancement Functions like magnification, brightness, and contrast were used. 13 landmarks (TABLE1) were used for linear measurements.
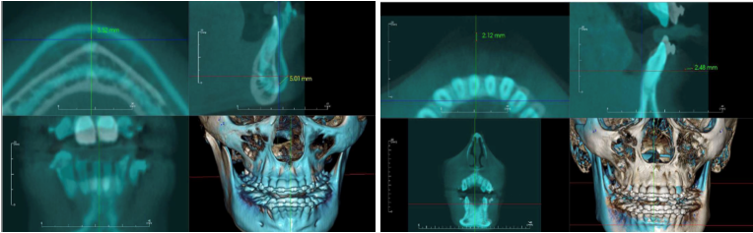
Method of 3-dimensional CBCT tracing: All the pre-operative and post-operative Dicom files were taken in anatomage Invivo 5.1 software(figure 4b), and superimposed by denoting or marking the pre-decided anatomical landmarks. The various measurements were then performed with the tools available in the software on superimposed data.
|
Structures |
Landmarks |
Definitions |
|
Maxilla |
ANS |
Anterior tip of the sharp bony process of the maxilla at the lower margin of the anterior nasal Opening |
|
|
PNS |
Posterior spine of the palatine bone constituting the hard palate |
|
|
A point |
Most posterior point of the curve of the maxilla, between ANS and the dental alveolus |
|
Mandible |
Gn |
Midpoint between the most anterior and inferior point on the bony chin |
|
|
Pg |
Most anterior point on the midsagittal symphysis of the Mandible |
|
|
B point |
Most posterior point in the concavity along the anterior border of the Mandibular symphysis. |
|
Dentition |
U1 Tip |
incisal tip of the upper central incisor |
|
|
U1 Apex |
tip of the root of upper central incisor |
|
|
L1 Tip |
incisal tip of the lower central incisor |
|
|
L1 Apex |
tip of the root of lower central incisor |
|
Soft tissue |
ST Pg |
Most anterior point on curve of soft tissue chin. |
|
|
ST Lower Lip |
Most anterior point on the curve of lower lip. |
|
|
ST Upper Lip |
Most anterior point on curve of the upper lip. |
|
ANS-ANS |
The linear distance between anterior nasal spine |
|
PNS-PNS |
The linear distance between posterior nasal spine |
|
A POINT- A POINT |
The linear distance between point A |
|
GN - GN |
The linear distance between gnathion |
|
PG – PG |
The linear distance between pogonion |
|
B POINT – B POINT |
The linear distance between point B |
|
U1 TIP – U1 TIP |
The linear distance between upper incisor tip |
|
U1 APEX – U1 APEX |
The linear distance between upper incisor apex |
|
L1 TIP – L1 TIP |
The linear distance between lower incisor tip |
|
L1 APEX - L1 APEX |
The linear distance between upper incisor apex |
|
ST Pg –ST Pg |
The linear distance between soft tissue Pogonion |
|
ST Lower Lip – ST Upper Lip |
The linear distance between soft tissue Upper lip |
|
ST Upper Lip – ST Lower Lip |
The linear distance between soft tissue lower lip |
Statistical analysis
The analysis was performed using SPSS statistical V 22.0 (version), IBM corporation; NY, USA) for MS Windows. The data on continuous variables were presented as Mean ± Standard deviation (SD). The statistical significance of the difference between the two superimposition methods was tested using one sample t-test with a reference difference of 1 mm, which was considered clinically significant. P-values less than 0.05 was considered to be statistically significant. All the hypotheses were formulated using two-tailed alternatives against each null hypothesis (hypothesis of no difference).
Results
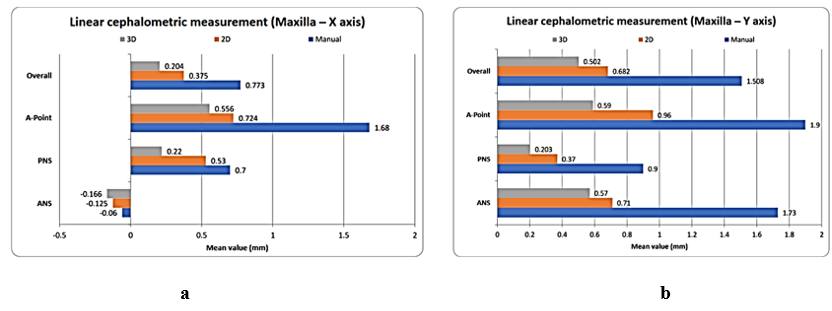
The study found that linear cephalometric measurements, including maxillary 2D and 3D measurements (excluding ANS and PNS), were significantly accurate compared to manual measurements. The 3D measurements were also significantly accurate compared to the 2D A-point measurements. The results suggest that these measurements are more accurate than manual ones.
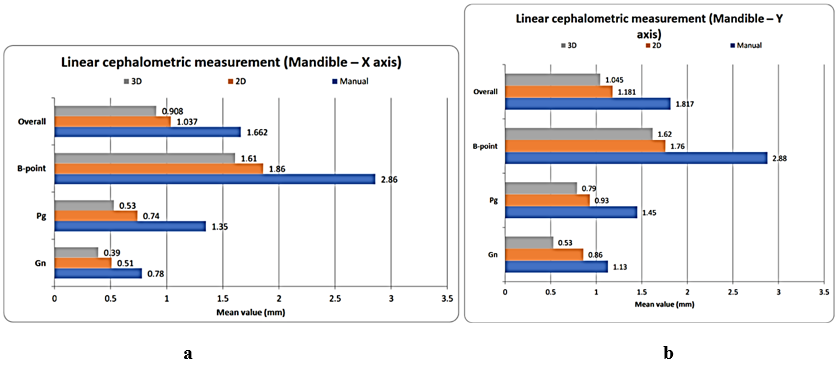
The study found that mandible 2D and 3D measurements, including Gn, Pg, and B-point, were significantly accurate compared to manual measurements (P-value<0.05) on the X-axis. Additionally, mandible 3D measurements were significantly accurate on the X-axis, and all Gn, Pg, and B-point measurements on the Y-axis were also significantly accurate.
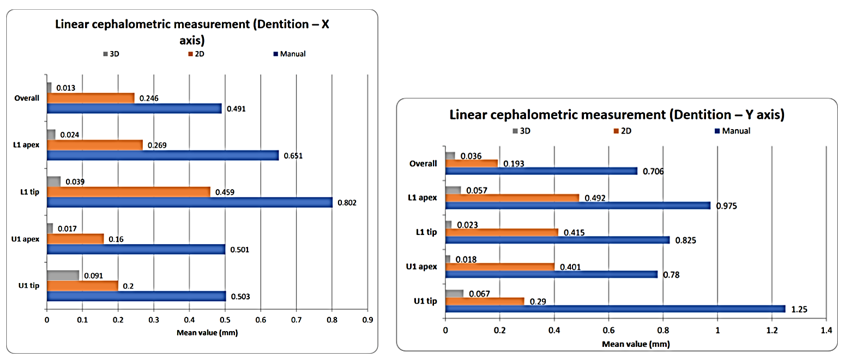
The measurements for landmarks of Dentition in 2D and 3D were found to be significantly more accurate than manual measurements, with X-axis and Y-axis measurements being the most accurate. (P-value<0.05)
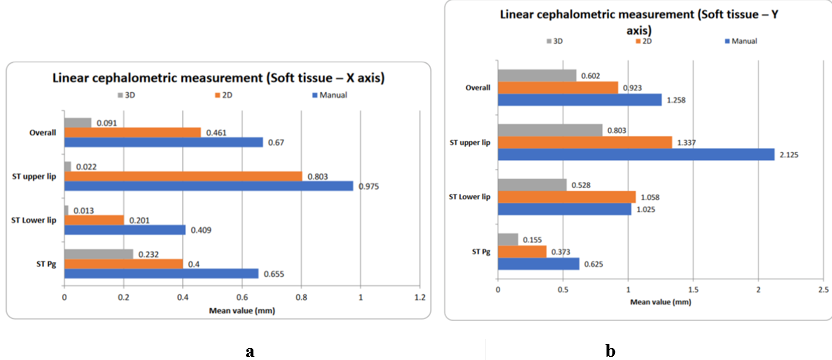
The study found that 3D soft tissue measurements were significantly accurate compared to manual and 2D measurements (P-value<0.05), while manual measurements did not significantly differ from 2D measurements (P-value>0.05).
Results Summary
The study found that linear cephalometric measurements were significantly accurate in various aspects of the body, including maxilla, mandible, dentition, and soft tissue.
Maxillary 2D and 3D measurements (excluding ANS and PNS) were significantly accurate compared to manual measurements, with 3D measurements being more accurate than 2D measurements.
Mandible measurements, such as Gn, Pg, and B-point, were also significantly accurate compared to manual measurements.
Dentition measurements were also significantly accurate compared to manual measurements, with 3D measurements being more accurate than 2D measurements.
Soft tissue measurements were also significantly accurate compared to manual and 2D measurements, with no significant difference in mean levels between manual and 2D measurements.
Discussion
Lateral cephalograms remain to be one of the orthodontic records which provide vital information about the sagittal and vertical relation of the craniofacial skeleton, soft tissue profile, dentition, airway and cervical vertebrae. The structures and their relationships to each other were analysed by means of linear and angular measurements as well as by the use of ratios based on the various cephalometric landmarks.[11] The diversity in landmark identification, measurement mistakes, and the conversion of three-dimensional objects to two-dimensional objects[6] are the sources of errors in hand tracing.[1], [2], [6], [12] The constraints of measurement tools (ruler and protractor)[9] and human visual performance in the case of manual tracing as reported by Forsyth et al.[10] defined the measurement of distances and angles between landmark sites.[10]
According to Sheldon Baumrind et al,[1] the main sources of inaccuracy in conventional cephalometric analysis are magnification, tracing, measuring, recording, and landmark identification and perceptual task involved in identifying landmarks varies from point to point.[1] To overcome this limitations, Computerized cephalometric devices were introduced into clinical orthodontics to address the drawbacks of the traditional tracing method. This method is widely used for diagnosis, therapy evaluation, and treatment outcome modelling. The method takes 10% as long as a typical manual registration because only the radiographic points directly on the cephalogram need to be digitalized.[8] The benefits are that the calculations are completed quickly. All human error is eliminated by this technique save for mistakes in landmark recognition. Computerized analysis can lessen the human errors made during manual measuring procedures, as demonstrated by Ssu - kuang Chen et al.[8] in their study.
In this study, there was no significant difference in landmarks ANS and PNS in manual, Maxillary 2D and 3D measurements (X-axis) (P-value 0.05). Compared to manual, mandible 2D measurements, there was no significant difference in mandibular landmark Gn (X-axis). Mandibular (X-axis) 2D and 3D measurements of Gn, Pg, and B-point were significantly more precise than manual measurements (P-value 0.05). When compared to manual measurements (X-axis and Y-axis), In Dentition 2D and 3D measurements (X-axis and Y-axis) were significantly more accurate (P-value 0.05). In comparison between the manual method and the digital method, there was no significant difference in landmarks which is in agreement with a study conducted by Dustin Roden.[13]
Another study was conducted by Georgios Tsorovas et al.[14] and Margherita Santoro et al[15] to evaluate the accuracy of cephalometric measurements obtained with digital tracing software compared with equivalent hand-traced measurements. They found that the digital method was more accurate then hand tracing method which is in agreement with this study.
Digital imaging offers advantages over traditional radiography,[8] such as quicker processing, reduced radiation dose by almost 30%,[10] and easier recognition of landmarks. However, it also requires a costly digital cephalometric radiography machine and associated software. Although digitalization converts analogue images into digital ones, it does not result in higher measurement inaccuracy compared to hand tracing.[15], [16] The growing popularity of digital cephalometrics has highlighted the need to assess the precision of new computerized software programs and compare them with traditional manual measuring methods.
Superimpositions based on digital data may not be reliable sometimes , according to a prior report by Harrell et al. This is because of the limitations of conventional 2D lateral cephalograms. Despite the fact that 3D CBCT cephalometry is thought to be very accurate and reliable.[7], [17]
The study found that maxillary 3D measurements were significantly more accurate than maxillary 2D measurements, and the 3D measurements of the maxillary A-point were more accurate than the 2D measurements. Mandible 3D measurements were also more accurate than manual measurements, and dentition 3D measurements were more accurate than dentition 2D measurements. These findings suggest that 3D measurements can improve the accuracy of dental procedures.
A study conducted by Shokori et al CBCT imaging values are more accurate indicators than calculated digital lateral cephalometry values because they are significantly closer to the actual distance which is in agreement with this study.[18]
Undistorted 3D morphology can be found in CBCT data sets, allowing for more accurate identification of craniofacial features. However, landmark identification in 3D is not simple. However, landmark identification in 3D is not simple. Attaining a high degree of precision is crucial, particularly in the context of novel instrumentation in science, as misinterpretations of images lead to incorrect diagnosis and, consequently, incorrect treatment strategies. Furthermore, there should be concerns that person who are inappropriately trained to read images, regardless of the method used, will misinterpret the data with consequent misdiagnoses and inappropriate patient treatment.
In this study , the sample size was relatively smaller with reference to the study published by J. Heinz et.al.[7] in the literature which could be the limitation of this study. However the sample size calculation showed statistical power more than 80% for 5% level of significance using the effect size published in the literature, we thus recommend further study to be conducted with relatively higher sample size .
Conclusion
Maxillary and mandibular measurements showed improved 3D accuracy over manual and 2D methods in both the X and Y axes. Dentition measurements significantly improved in 2D and 3D compared to manual. Soft tissue measurements in 3D surpassed both manual and 2D, with no significant difference from 2D for mean soft tissue measurements. Compared to manually and digitally traced radiographs, all evaluated procedures were acceptable and dependable. The CBCT scans provided higher levels of accuracy and reliability.
|
Abbreviation |
Full form |
|
CBCT |
Cone beam computed tomography |
|
2D |
Two dimensional |
|
3D |
Three dimensional |
|
KVp |
Kilovoltage |
|
MA |
Milliampere |
|
cm |
Centimetre |
|
mm |
Millimeter |
|
mins |
Minutes |
|
jpeg |
Joined photographic experts group |
|
Ans |
Anterior nasal spine |
|
Pns |
posterior nasal spine |
|
Gn |
gnathion |
|
Pg |
pogonion |
|
U1 |
Upper incisors |
|
L1 |
Lower incisors |
|
St pog |
Soft tissue pogonion |
|
S |
Sella |
|
N |
Nasion |
|
po |
Pogonion |
|
O |
Orbitale |
|
Ptm |
pterygoid |
|
Ba |
basion |
|
Dicom |
Digital imaging and communication in medicine |
|
NS |
Non-significant |
|
Anova |
Analysis of variant |
Copyright Releases
"The undersigned author transfers all copyright ownership of the manuscript – (Comparative Evaluation Of Accuracy For Manual, Digital And Cbct Generated Superimposition Of Cephalometric Landmarks- A Retrospective Study) - to The Angle Orthodontist in the event the work is published. The undersigned author warrants that the article is original, is not under consideration for publication by another journal and has not been previously published. I sign for and accept responsibility for releasing this material on behalf of any and all coauthors."
Ethical Approval
Study is approved by ethical committee of institute and MUHS research committee.
Source of Funding
None.
Conflict of Interest
None.
Acknowledgement
I would like to express my sincere gratitude to my mentor and guide Dr. Ajit Kalia (HOD and Professor, Department of Orthodontics, M. A. Rangoonwala College of Dental Science and Research Centre, Pune) who provided inspiration and guidance behind the idea of the study.
References
- S Baumrind, RC Frantz. The reliability of head film measurements: 1. Landmark identification.. Am J Orthod 1971. [Google Scholar]
- R M Ricketts. . Perspectives in the clinical application of cephalometrics: the first fifty years. The Angle Orthodontist 1981. [Google Scholar]
- A M Vincent, V C West. Cephalometrick landmark identification error. Australian orthodontic journal 1987. [Google Scholar]
- S Asif, M Tariq. Methods of cephalometric superimposition-A review. Indian Journal of Orthodontics and Dentofacial Research 2016. [Google Scholar]
- J H Moon, H W Hwang, S J Lee. . Evaluation of an automated superimposition method for computer-aided cephalometrics. The Angle Orthodontist 2020. [Google Scholar]
- P J Sandler. . Reproducibility of cephalometric measurements. British journal of orthodontics 1988. [Google Scholar]
- J Heinz, K Stewart, A Ghoneima. Evaluation of two-dimensional lateral cephalogram and three-dimensional cone beam computed tomography superimpositions: a comparative study. Int J Oral Maxillofac Surg 2019. [Google Scholar]
- SK Chen, YJ Chen, CC Yao, HF Chang. Enhanced speed and precision of measurement in a computer-assisted digital cephalometric analysis system. . Angle Orthod 2004. [Google Scholar]
- M Berco, JR Rigali, PH Miner, RM Deluca, S Anderson, NK Will. Accuracy and reliability of linear cephalometric measurements from cone-beam computed tomography scans of a dry human skull. Am J Orthod Dentofac Orthop 2009. [Google Scholar]
- DB Forsyth, DN Davis. Assessment of an automated cephalometric analysis system. Eur J Orthod 1996. [Google Scholar]
- NM Helal, OA Basri, HA Baeshen. Significance of cephalometric radiograph in orthodontic treatment plan decision. J Contemp Dent Pract 2019. [Google Scholar]
- AM Cohen. Uncertainty in cephalometrics. . Brit J Orthod 1984. [Google Scholar]
- DR Johnson, J English, R Gallerano. Comparison of hand-traced and computerized cephalograms: landmark identification, measurement, and superimposition accuracy. Am J Orthod Dentofac Orthop 2008. [Google Scholar]
- G Tsorovas, A Linder-Aronson Karsten. A comparison of hand-tracing and cephalometric analysis computer programs with and without advanced features-accuracy and time demands. . Eur J Orthod 2010. [Google Scholar]
- M Santoro, K Jarjoura, T J Cangialosi. Accuracy of digital and analogue cephalometric measurements assessed with the sandwich technique. American Journal of Orthodontics and Dentofacial Orthopedics 2006. [Google Scholar]
- RD Navarro, PV Oltramari-Navarro, TM Fernandes, GF Oliveira, AC Conti, MR Almeida. Comparison of manual, digital and lateral CBCT cephalometric analyses. J Appl Oral Sci 2013. [Google Scholar]
- RM Nada, TJ Maal, KH Breuning, SJ Berge, YA Mostafa, AM Kuijpers-Jagtman. Accuracy and reproducibility of voxel based superimposition of cone beam computed tomography models on the anterior cranial base and the zygomatic arches. . PloS one 2009. [Google Scholar]
- A Shokri, S Khajeh, A Khavid. Evaluation of the accuracy of linear measurements on lateral cephalograms obtained from cone-beam computed tomography scans with digital lateral cephalometric radiography: an in vitro study. J Craniofac Surg 2014. [Google Scholar]