- Visibility 12 Views
- Downloads 7 Downloads
- DOI 10.18231/j.jco.2024.031
-
CrossMark

Beyond the ARCH: Examining mandibular third molar movements in response to premolar and single incisor extractions in orthodontic practice
- Author Details:
-
 Swaroopa Rani Ponnada *
Swaroopa Rani Ponnada *
-
Sharmila Kantheti
-
Chandrasekhar Gandikota
-
Ranjit Manne
Introduction
The eruption of the mandibular third molar (M3) and their influence on the dental arch has long been a subject of controversy that interests various specialties of dentistry.[1]
The impaction rate for the third molar (M3) is higher than any other tooth, approaching 24% worldwide. M3 impaction is more frequently observed in the mandible than in the maxilla.[2]
Third molars possess a diverse array of characteristics, including varying shapes, sizes, positions, root formations, and eruption pathways.
There are various hypotheses presumed for impaction of 3rd molars, these include as the bud of the third molar emerges and comes into contact with the second molar, it undergoes significant pre-eruptive rotational movements and angular positioning. These movements and positions continue even after the third molars have fully emerged, causing crowding in the front lower jaw.[3]
The inadequate space behind the molars and limited jaw bone remodelling can present challenges for the eruption of third molars. Additionally, the absence of periosteal growth on the maxillary tuberosity can also hinder the emerging of maxillary third molars.[4], [5] due to natural attrition between neighbouring teeth which allowed for drifting of the posterior teeth, lack of proper uprightness during the process of root formation often results in third molar impaction, particularly more frequently in the lower jaw rather than the upper.[6]
Third molars can appear on radiographs as early as 5 or as late as 16 years. Initially, lower third molars show mesial inclination, becoming more upright until age 25, often erupting between 18 and 24 years.[7]
Various studies have been validated to substantiate the association between premolar extraction treatment, mesial molar movement, and increased eruption space for third molars.[8], [9], [10]
Hence, the present study has been taken up to see for the possibility of co-relation between extraction pattern and M3 angulation.
Materials and Methods
A total of thirty samples of Orthopantomograms (pre-treatment & post-treatment) of patients who have reported to the centre seeking for an orthodontic treatment have been collected.
These were divided into 2 groups
-Group I including Premolar extractions
-Group II including Single incisor extractions
This study was conducted after obtaining an ethical clearance from the institution (IEC No: PMVIDS & RC/IEC/ORTHO/PR/547-22)
The orthopantomograms of patients included in this study were of Asian ethnicity & South Indian demography.
The inclusion criteria include
Panoramic radiographs at T0 & T1 of patients with formulated treatment plan of extraction of premolars and single incisor. [5]
The exclusion criteria include
1. Patients were excluded if the 3rd molars at T0 had already erupted
2. Any dental abnormalities (hypo-/ hypodontia, [3] impaction, dental transposition,[1], microdontia, or cysts), distalization mechanics, congenital malformations, [9] or syndromes.[11]
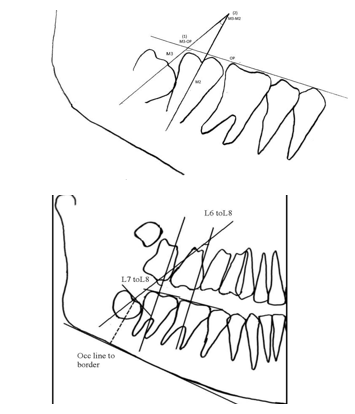
Panoramic radiographs (T0 and T1) were assessed using a standardized technique involving tracing the tooth outlines (premolars and molars) on matte acetate paper.

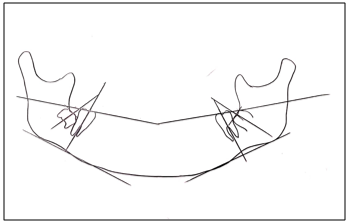
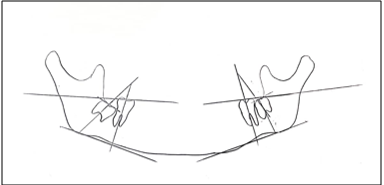
The line connecting the mesiobuccal cusps of the first molar with the buccal cusps of the second premolar defined the occlusal plane (OP): (M3–OP)
Two angular measurements were measured as described below:
1. The angle between the long axis of the third molar (M3) (line bisecting the line connecting the mesial and distal outlines of the cervical areas)
2. The angle between the long axis of the second molar (M2) (midocclusal point through the midpoint of the root bifurcation and the midpoint between the mesial and distal root tips) and the long axis of the third molar: (M3–M2)[1]
The impaction rate for the third molar (M3) is higher
than any other tooth, approaching 24% worldwide.
1M3 impaction is more frequently observed in the mandible
than in the maxilla.
The impaction rate for the third molar (M3) is higher
than any other tooth, approaching 24% worldwide.
1 M3 impaction is more frequently observed in the mandible than in the maxilla.
The impaction rate for the third molar (M3) is higher
than any other tooth, approaching 24% worldwide.
1 M3 impaction is more frequently observed in the mandible than in the maxill
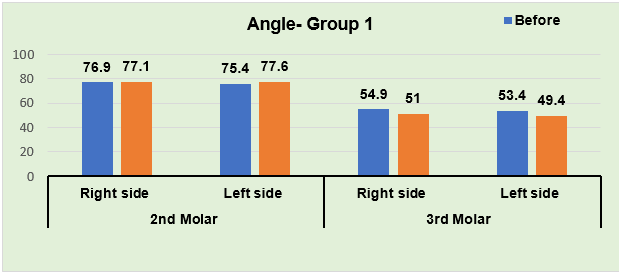
Results
The angular measurements of 2nd and 3rd molars and linear measurement of 3rd molar to assess the positional changes on both left and right sides were entered into a master excel sheet and descriptive statistical analysis was performed.
|
Mand. Molar |
Side |
Timeline |
n |
Mean |
SD |
Test statistic |
P value |
|
2nd Molar |
Right side |
Before |
15 |
76.9333 |
4.46361 |
-0.228 |
0.820 |
|
After |
15 |
77.1333 |
8.28826 |
||||
|
Left side |
Before |
15 |
75.4667 |
6.20906 |
-1.155 |
0.248 |
|
|
After |
15 |
77.6000 |
6.06865 |
||||
|
3rd Molar |
Right side |
Before |
15 |
54.9333 |
22.37175 |
-1.307 |
0.191 |
|
After |
15 |
51.0667 |
27.47588 |
||||
|
Left side |
Before |
15 |
53.4000 |
19.78383 |
-1.382 |
0.167 |
|
|
After |
15 |
49.4667 |
22.73093 |
|
Mand. Molar |
Side |
Timeline |
n |
Mean |
SD |
Test statistic |
P value |
|
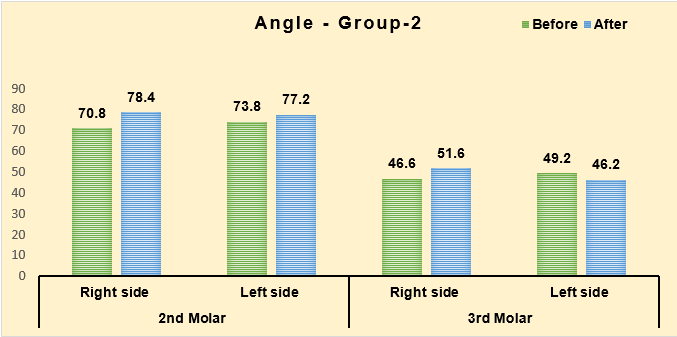
2nd Molar |
Right side |
Before |
15 |
70.8667 |
9.53090 |
-2.661 |
0.008* |
|
After |
15 |
78.4667 |
5.65517 |
||||
|
Left side |
Before |
15 |
73.8000 |
5.73461 |
-2.091 |
0.036* |
|
|
After |
15 |
77.2000 |
3.14416 |
||||
|
3rd Molar |
Right side |
Before |
15 |
46.6000 |
15.72441 |
-0.654 |
0.513 |
|
After |
15 |
51.6000 |
20.64600 |
||||
|
Left side |
Before |
15 |
49.2667 |
15.86310 |
-1.260 |
0.208 |
|
|
After |
15 |
46.2000 |
17.39951 |
|
Mand. Molar |
Side |
Timeline |
n |
Mean |
SD |
Test statistic |
P value |
|
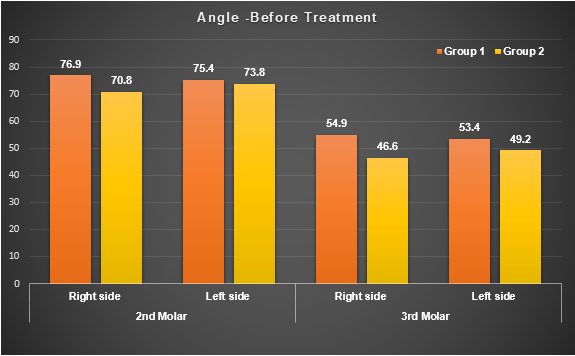
2nd Molar |
Right side |
Group 1 |
15 |
76.9333 |
4.46361 |
-2.038 |
0.042* |
|
Group 2 |
15 |
70.8667 |
9.53090 |
||||
|
Left side |
Group 1 |
15 |
75.4667 |
6.20906 |
-0.542 |
0.588 |
|
|
Group 2 |
15 |
73.8000 |
5.73461 |
||||
|
3rd Molar |
Right side |
Group 1 |
15 |
54.9333 |
22.37175 |
-1.662 |
0.097 |
|
Group 2 |
15 |
46.6000 |
15.72441 |
||||
|
Left side |
Group 1 |
15 |
53.4000 |
19.78383 |
-0.936 |
0.350 |
|
|
Group 2 |
15 |
49.2667 |
15.86310 |
|
Mand. Molar |
Side |
Timeline |
n |
Mean |
SD |
Test statistic |
P value |
|
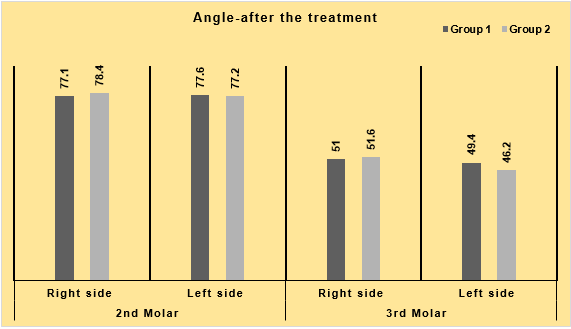
2nd Molar |
Right side |
Group 1 |
15 |
77.1333 |
8.28826 |
-0.354 |
0.744 |
|
Group 2 |
15 |
78.4667 |
5.65517 |
||||
|
Left side |
Group 1 |
15 |
77.6000 |
6.06865 |
-0.356 |
0.722 |
|
|
Group 2 |
15 |
77.2000 |
3.14416 |
||||
|
3rd Molar |
Right side |
Group 1 |
15 |
51.0667 |
27.47588 |
-0.187 |
0.852 |
|
Group 2 |
15 |
51.6000 |
20.64600 |
||||
|
Left side |
Group 1 |
15 |
49.4667 |
22.73093 |
-0.832 |
0.406 |
|
|
Group 2 |
15 |
46.2000 |
17.39951 |
|
Mand. Molar |
Side |
Timeline |
n |
Mean |
SD |
Test statistic |
P value |
|
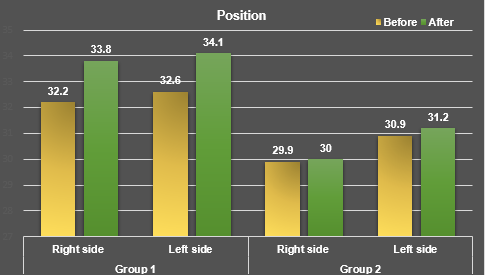
3rd Molar |
Right side |
Before |
15 |
32.2000 |
6.10854 |
-1.203 |
0.249 |
|
After |
15 |
33.8667 |
4.22352 |
||||
|
Left side |
Before |
15 |
32.6000 |
4.71775 |
-1.239 |
0.236 |
|
|
After |
15 |
34.1333 |
4.10342 |
|
Mand. Molar |
Side |
Timeline |
n |
Mean |
SD |
Test statistic |
P value |
|
3rd Molar |
Right side |
Before |
15 |
29.9333 |
4.02611 |
-0.202 |
0.812 |
|
After |
15 |
30.0667 |
4.09646 |
||||
|
Left side |
Before |
15 |
30.9333 |
3.19523 |
-0.357 |
0.727 |
|
|
After |
15 |
31.2667 |
4.00832 |
|
Mand. Molar |
Side |
Timeline |
n |
Mean |
SD |
Test statistic |
P value |
|
3rd Molar |
Right side |
Group 1 |
15 |
32.2000 |
6.10854 |
1.200 |
0.240 |
|
Group 2 |
15 |
29.9333 |
4.02611 |
||||
|
Left side |
Group 1 |
15 |
32.6000 |
4.71775 |
1.133 |
0.268 |
|
|
Group 2 |
15 |
30.9333 |
3.19523 |
|
Mand. Molar |
Side |
Timeline |
n |
Mean |
SD |
Test statistic |
P value |
|
3rd Molar |
Right side |
Group 1 |
15 |
33.8667 |
4.22352 |
2.501 |
0.018* |
|
Group 2 |
15 |
30.0667 |
4.09646 |
||||
|
Left side |
Group 1 |
15 |
34.1333 |
4.10342 |
1.936 |
0.063 |
|
|
Group 2 |
15 |
31.2667 |
4.00832 |
Discussion
Predicting third molar eruption during orthodontic treatment can prevent the future insight of impactions, thereby addressing the clinical challenge associated with third molar impaction.[12]
Measurements of third molar angulation on lateral cephalograms, as seen in previous studies, [6], [8] may be biased because of the differences in the angulation between the superimposed images. Overcoming issues in cephalometric studies of posterior tooth position changes requires measurements on 60-degree head films of both left and right sides, as demonstrated by Richardson [13] Hence opgs are taken into account in the present study.
There are some factors that influence the eruption of mandibular 3rd molars during calcification, mandibular third molar buds’ angle mesially, while maxillary buds’ angle distally. Richardson [13] noted a 11.2⁰ average displacement in mandibular third molars between 10 and 15 years, suggesting a tendency for uprighting. Failure in rotational movements may lead to impaction, but some authors propose that extracting mesially positioned teeth can stimulate uprighting rotational movements.[14]
According to various studies, extracting premolars as part of treatment may result in a significant shift of the third molar towards the front of the mouth, while not extracting premolars may lead to a significant increase in the likelihood of the third molar becoming impacted. However, there are differing opinions on this matter, as some researchers have found no noteworthy variances in patients who received treatment with or without premolar extractions.[15]
However, in contrast, Haavikko [16] argues that while premolar extractions do have the effect of accelerating the eruption of teeth, they do not necessarily promote the eruption of wisdom teeth.[17]
In a study conducted by Saysel et.al. have concluded that the changes in angulation of mandibular third molars in the extraction group were significantly more upright.[18]
In a study conducted by Gohilot et.al. [19] A significant improvement in maxillary third molar angulation following extraction treatment was seen on both the right and left sides, however there was no change in the angulation of mandibular 3rd molar was seen in extraction group which was similar to study by Turkoz C et.al. [20]
In contrary to the above studies significant relationship was observed between the initial age of the patient and the amount of change in the inclination of the third molar in a study by Schiller et.al. [21]
There is gender-specific variations in the angulation of third molars, demonstrating a higher degree of verticalization in women compared to men [22] As with previous M3 studies, the present study did not reveal a basis to predict the eruption of M3. [23]
In a study conducted by Al kuwari etal it was concluded that the orthodontic treatment involving first premolar extraction has shown improvement in the angulation of third molars during eruption, thereby supporting the implementation of orthodontic extraction therapy in borderline cases. [24]
In the present study 30 orthopantomograms were taken at T0 and T1 and analysed for positional and angulation changes in mandibular 3rd molars in premolar and single incisor extractions. These were categorized into 2 groups- Group I including premolar extractions & Group II including single incisors.
In comparison between both left and right sides at T0 & T1 there was no significant change in the angular changes of 3rd molars similar to those studies conducted by Saysel etal, Turkoz C etal, and contrary to studies by Al kuwari et.al., Schiller et.al.
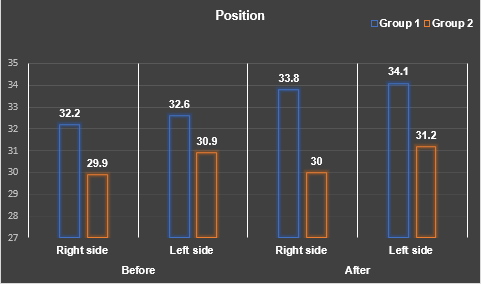
However, the present study showed there was statistically significant corelation on the position of mandibular 3rd molar post treatment in comparison to pre-treatment.
The limitations of the present study are that interpreting measurements from dental panoramic tomograms requires caution due to varying vertical and horizontal magnification. Insignificant angulation changes in third molars imply additional factors at play, such as anchorage, impaction type, tooth angulation, treatment duration, and age. These variables contribute to data variability and bias, potentially impacting research results.
Conclusion
Extracting the first premolar has a positive impact on the available space for the third molar to properly emerge. This implies that removing the first premolar allows for additional room, making it easier for the third molar to come through. However, it's worth noting that the study specifically evaluated the third molars' angle and position. While this offers valuable insight, it also recognizes the limitation of not considering other potential factors.
Factors such as dental asymmetry, premature contacts (teeth coming together before they should), and uncontrolled tipping (teeth leaning or tilting) are crucial elements that can influence the overall success of orthodontic treatment involving premolar extraction and impact the final positioning of the third molars
This research highlights the need for a more comprehensive assessment in future studies.
The study emphasizes that while first premolar extraction contributes positively to space management for third molars, a more thorough examination of various dental parameters is essential to draw more conclusive and comprehensive findings.
Source of Funding
None.
Conflict of Interest
None.
References
- B H Durgesh, K H Gowda, O A Alshahrani, A D Almalki, W D Almalki, M M Balharith, N Y Motashesh, A A Alkheraif, M I Hashem. Influence of premolar extraction or non-extraction orthodontic therapy on the angular changes of mandibular third molars. Saudi Journal of Biological Sciences 2016. [Google Scholar]
- Mang De La Rosa, M R Langer, L J Kouroupakis-Bakouros, F Jost-Brinkmann, P G Bartzela, T N. . Angular and positional changes of the maxillary third molars after orthodontic treatment with different premolar extraction patterns. The Angle Orthod 2023. [Google Scholar]
- R Oksayan, T Topcuoglu. Effects of mandibular third molar angulation and position on crowding. Turk J Orthod 2013. [Google Scholar]
- B H Faubion. Effect of extraction of premolars on eruption of mandibular third molars. J. Am. Dent. A 1968. [Google Scholar]
- S Velachery, S Backer, S Shetty, K Parveen, N K Shetty, A Husain. Angular changes of impacted mandibular third molars and developing mandibular third molars in premolar extraction cases- A retrospective radiographic study. Int J Oral Health Dent 2021. [Google Scholar]
- J Artun, L Thalib, R M Little. Third molar angulation during and after treatment of adolescent orthodontic patients. Eur. J. Orthod 2005. [Google Scholar]
- M J Elsey, W Rock. Influence of orthodontic treatment on development of third molars. British Journal of Oral and Maxillofacial 2000. [Google Scholar]
- T W Kim, J Artun, F Behbehani, F Artese. Prevalence of third molar impaction in orthodontic patients treated non-extraction and with extraction of 4 premolars. Am. J. Orthod. Dentofacial Orthop 2003. [Google Scholar]
- B Russell, M Skvara, E Draper, W R Proffit, C Philips, R P White. . The association between orthodontic treatment with removal of premolars and the angulation of developing mandibular third molars over time. The Angle Orthod 2013. [Google Scholar]
- D D Dierkes. An investigation of the mandibular third molars in orthodontic cases. Angle Orthod 1975. [Google Scholar]
- S Singh, A K Garg, D K Gupta. Changes in Mandibular Third Molar Angulation in High-anchorage Extraction vs Non-extraction Orthodontic Treatment: A Prospective Study. J Contemp Dent Pract 2020. [Google Scholar]
- S Jain, A Valiathan. Influence of first premolar extraction on mandibular third molar angulation. Angle Orthod 2009. [Google Scholar]
- M E Richardson, M Dent. Some aspects of lower third molar eruption. Angle Orthod 1974. [Google Scholar]
- G Silling. Development and eruption of the mandibular third molar and its response to orthodontic therapy. Angle Orthod 1973. [Google Scholar]
- B Tarazona, V Paredes, JM Llamas. Influence of first and second premolar extraction or non-extraction treatments on mandibular third molar angulation and position. A comparative study. Med Oral Patol Oral Cir Bucal 2010. [Google Scholar]
- K Haavikko, M Altonen, K Mattila. Predicting angulational development and eruption of the lower third molar. Angle Orthod 1978. [Google Scholar]
- AM Mihai, IR Lulache, R Grigore, AS Sanabil, S Boiangiu, E Ionescu. Positional changes of the third molar in orthodontically treated patients. J Med Life 2013. [Google Scholar]
- MY Saysel, GD Meral, I Kocadereli, F Tasar. The effects of first premolar extractions on third molar angulations. Angle Orthod 2005. [Google Scholar]
- A Gohilot, T Pradhan, KM Keluskar. Effects of first premolar extraction on maxillary and mandibular third molar angulation after orthodontic therapy. J Oral Biol Craniofac Res 2012. [Google Scholar]
- C Türköz, C Ulusoy. Effect of premolar extraction on mandibular third molar impaction in young adults. Angle Orthod 2013. [Google Scholar]
- WR Shiller. Positional changes in mesio-angular impacted mandibular third molars during a year. J Am Dent Assoc 1979. [Google Scholar]
- LV Mendoza-García, EV Jiménez, AG Rocha. Effect of orthodontic treatment involving first premolar extractions on mandibular third molar angulation and retromolar space. J Clin Exp Dent 2017. [Google Scholar]
- FN Hattab. Positional changes and eruption of impacted mandibular third molars in young adults. A radiographic 4-year follow-up study. . Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997. [Google Scholar]
- RM Albadr, HM Talakey, AA Al-Sahli, . Influence of orthodontic treatment with first premolar extraction on the angulation of the mandibular third molar. Saudi Med J 2013. [Google Scholar]